
More Information
Submitted: May 24, 2022 | Approved: June 03, 2022 | Published: June 06, 2022
How to cite this article: Cherni N, Chaachou A, Ferjaoui W, Dridi M, Ghozzi S. Cutaneous metastasis of a tumor of the excretrial tract. Arch Case Rep. 2022; 6: 015-016.
DOI: 10.29328/journal.acr.1001060
Copyright License: © 2022 Cherni N, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Cutaneous metastasis of a tumor of the excretrial tract
Nizar Cherni1, Abdallah Chaachou1, Wael Ferjaoui2*, Mohamed Dridi1 and Samir Ghozzi1
1Department of Urology, Military Hospital of Tunis, Tunisia
2Department of General Surgery, Military Hospital of Tunis, Tunisia
*Address for Correspondence: Wael Ferjaoui, Department of General Surgery, Mongi Slim University Hospital, Faculty of Medicine of Tunis, Email: [email protected]
Cutaneous metastases of urothelial tumors are extremely rare. Iatrogenic tumor implantations are the main cause of this type of metastasis. We report the case of a 75-year-old patient who underwent nephroureterectomy with the removal of a bladder collarette for a tumor of the upper excretory tract; 3 years later the patient developed parietal swelling at the level of the lumbotomy scar. A histological study of the mass after surgical excision confirmed that it was a secondary location. Through a study of the literature, we will detail the clinical and paraclinical particularities of such a location as well as its impact on the prognosis.
A 75-year-old patient with no particular history was hospitalized in July 2001 for isolated total hematuria with no deterioration in general condition. The clinical examination was normal. Biology: no kidney failure. The computed tomography showed a tumoral process occupying the upper clinical group of the right kidney (Figure 1). In August 2001 a nephroureterectomy with the removal of a bladder collarette was performed. The postoperative course was uneventful. Histology showed: well-differentiated (grade 1), non-invasive
transitional cell papillary carcinoma of the pyelo-calicielle cavities of the right kidney. In April 2002 the patient presented a haematuric recurrence, he underwent a resection of a unifocal bladder tumor. The histology concluded a superficial urothelial carcinoma. In October 2005 the patient was hospitalized for a solid parietal swelling (Figure 1) at the level of the lumbotomy scar with a long axis of 7 cm. On the abdominopelvic: no tumor recurrence; the presence of a parietal mass taking up the contrast in a heterogeneous tissue-like manner, probably the site of necrosis. En bloc excision of the tumor was performed. Histology revealed parietal metastasis of urothelial carcinoma (Figure 2). 6 months later, the patient was re-hospitalized for a recurrence at the same location of this 25 cm tumor mass which seemed fixed in relation to the deep plane. Since the tumor could not be removed surgically this time, chemotherapy was indicated for this patient.

Figure 1: A solid parietal swelling at the level of the lumbotomy scar with a long axis of 7 cm.
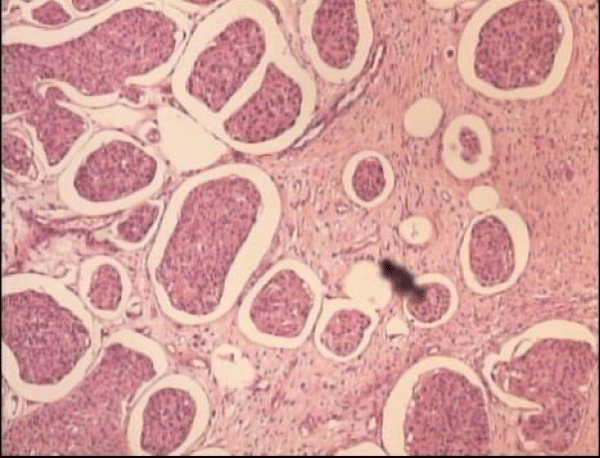
Figure 2: Histology revealed parietal metastasis of a urothelial carcinoma.
Urinary tumors are rarely responsible for skin metastases [1]. The usual sites of metastases are essentially the lymph nodes, bone, liver, and lungs [2]. The mechanisms of dissemination are direct tumor invasion by contiguity, iatrogenic implantation of the surgical site, and lymphatic or hematogenous dissemination. Clinically, these cutaneous metastases appear either as nodules or inflammatory lesions or as fibrous and scar-like tumor masses. The prognosis of these patients is poor with a survival < 6 months. The treatment is essentially palliative, surgery alone or sometimes combined with radio-chemotherapy [3,4].
- Muellera TJ, Wub H, Greenberga RE, Hudesc G, Tophamd N, Lessinc SR, Uzzo RG. Urology. 2004; 63:1021-1026.
- Gates O. Cutaneous metastases of malignant disease. Am J Cancer. 1937; 30:718-730.
- Tinkle LL, Graham BS, Spillane TJ, Barr RJ. Testicular choriocarcinoma metastatic to the skin: an additional case and literature review. Cutis. 2001 Feb;67(2):117-20. PMID: 11236220.
- Dorairajan LN, Hemal AK, Aron M, Rajeev TP, Nair M, Seth A, Dogra PN, Gupta NP. Cutaneous metastases in renal cell carcinoma. Urol Int. 1999;63(3):164-7. doi: 10.1159/000030440. PMID: 10738187.