
More Information
Submitted: April 28, 2022 | Approved: May 23, 2022 | Published: May 24, 2022
How to cite this article: Ayadi MF, Atallah A, Medhioub F, Omrani S, Ferjaoui W, et al. Incidental discovery of a pancreatic lipoma: a case report. Arch Case Rep. 2022; 6: 013-014.
DOI: 10.29328/journal.acr.1001059
Copyright License: © 2022 Ayadi MF, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Incidental discovery of a pancreatic lipoma: a case report
Mohamed Firas Ayadi1,2, Aziz Atallah1,2, Fatma Medhioub1,2,
Sahir Omrani1,2, Wael Ferjaoui1,2* *, Hafedh Mestiri1,2 and Rached Bayar1,2
*, Hafedh Mestiri1,2 and Rached Bayar1,2
1Department of General Surgery, Mongi Slim University Hospital, Tunis, Tunisia
2Faculty of Medicine of Tunis, Tunis El Manar University, Tunis, Tunisia
*Address for Correspondence: Wael Ferjaoui, Department of General Surgery, Mongi Slim University Hospital, Faculty of Medicine of Tunis, Email: [email protected]
Pancreatic lipoma is a benign, mesenchymal-derived tumor. It is an uncommon entity that is rarely reported. The diagnosis is usually made on a CT scan or MRI. We present a case of a pancreatic lipoma incidentally discovered on imaging in a 53-years old patient presenting for acute cholecystitis.
Pancreatic lipoma is a benign tumor of mesenchymal origin [1]. This is an exceptional entity. Indeed in the literature, less than 180 cases are reported since it is first discovered [2,3]. Its preferential location is the head of the pancreas [1]. This entity is exceptionally symptomatic and usually discovered on imaging [4].
The particularity of this tumor is that sometimes it is difficult to distinguish it from a well-differentiated liposarcoma [3].
We report the case of a patient who presented for acute cholecystitis in whom a pancreatic lipoma was discovered.
A 53-year-old patient with no significant past medical history presented in for fiver and right upper abdominal quadrant pain that has been evolving for 4 days. The physical examination revealed a temperature of 39 °C, blood pressure of 130/70 mmHg, a pulse of 110 BPM, and a right upper quadrant guarding. There was no jaundice.
The results of laboratory tests revealed a WBC at 15300/mm3 and a C-reactive protein at 116 mg/L. There was no cholestasis or cytolysis and blood lipase was normal. The rest of the laboratory values were within normal.
The diagnosis of acute cholecystitis was suspected and an abdominal ultrasound was performed. It showed an aspect of acute lithiasis cholecystitis: a distended gallbladder with a thick laminated wall and lithiasis content. We also note the presence of a fatty mass of the head of the pancreas of 2 cm.
An abdominal CT scan was performed and concluded a pancreatic lipoma by showing a fatty mass of the head of the pancreas measuring 23 mm on the long axis. It was homogeneous without calcification or contrast uptake. It also confirmed the diagnosis of the cholecystitis (Figures 1,2).
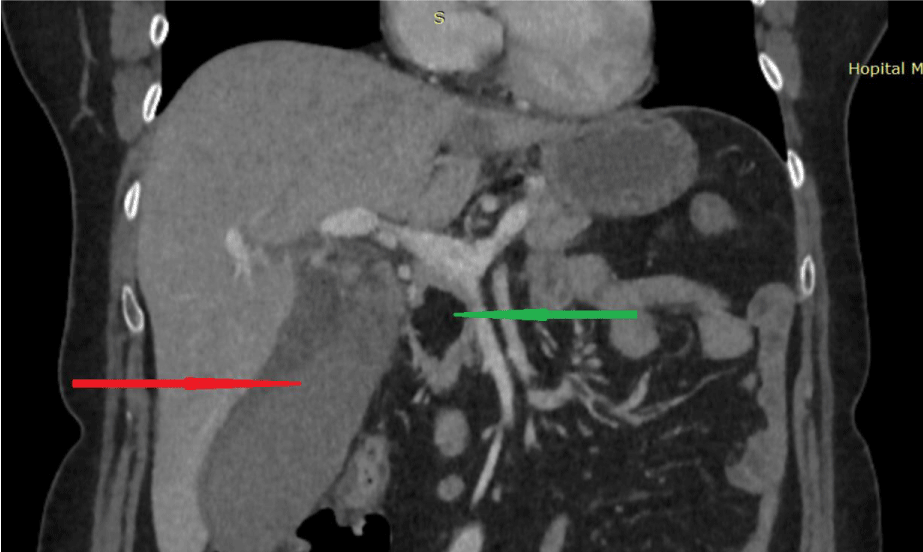
Figure 1: The pancreatic lipoma (green arrow) homogenous fatty mass of the head of the pancreas with no contrast enhancement and no pancreatic infiltration. Distended gallbladder with peritoneal effusion, confirming the cholecystitis (red arrow).
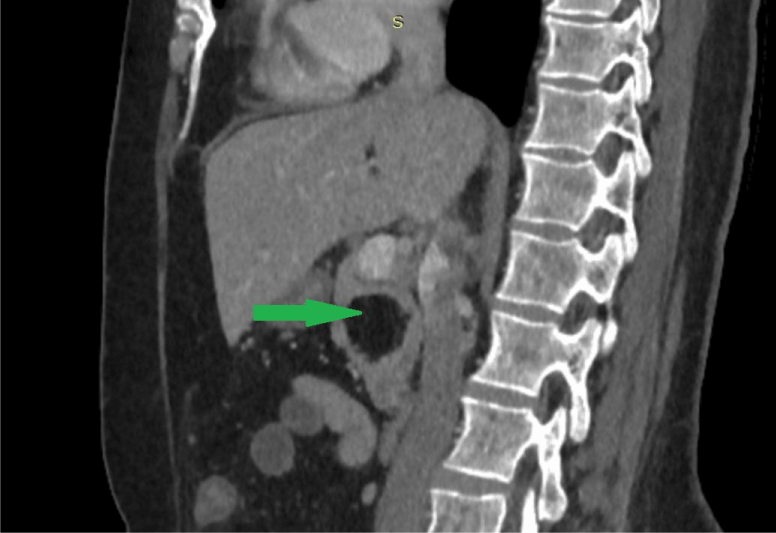
Figure 2: Lipoma of the head of the pancreas (green arrow).
The patient had a laparoscopic cholecystectomy with simple outcomes and was discharged on day 02 postoperatively.
For the pancreatic lipoma, we opted for surveillance, and an abdominal CT scan is planned for 3 months.
Pancreatic lipoma is a benign tumor of mesenchymal origins. Those tumors present only from 1% to 2% of all pancreatic tumors [1]. It was first reported on ultrasound imaging by Bigard, et al. in 1989 [4]. Since then, less than 180 cases were reported and most of them in china [2-4].
Its pathogenesis is still unclear and it mostly occurs in the head of the pancreas [1]. For that location, it is considered by some authors as an adipose tissue that was trapped during pancreas rotation [3]. Its transformation into liposarcoma is still uncertain [5].
It is usually asymptomatic and incidentally discover on imaging [6]. However, lipoma of the head of the pancreas can cause jaundice by compressing the ampulla of Vater [2] or a duodenal obstruction [1].
The diagnosis is usually made on a CT scan. In fact, Lehmann and al defined the CT findings it includes a homogenous distribution of fat density, no central or peripheral contrast enhancement, Housefield units of -80 to -120, and a sharp demarcation with no intra- and extra-pancreatic infiltration [2]. MRI can be a good help in doubtful cases and lipoma appears hyperintense on t1 and t2 similar to the abdominal and subcutaneous fat and with no contrast enhancement [7].
The differential diagnoses of this entity are focal fatty infiltration, pseudohypertrophic lipomatosis, teratoma, and liposarcoma [1]. In the case of typical images, histological confirmation is not required [7,8]. In case of doubt, an endoscopic transduodenal biopsy can guide the management [1].
Considering its rarity there are no established guidelines for the management of this tumor [4]. However asymptomatic lipomas require follow-up [1]. This is justified by the fact that its transformation into liposarcoma is still uncertain [5].
For the symptomatic forms, surgery is required and it is depending on the location of the lipoma and the intraoperative findings [1]. It can vary from simple excision to a Whipple’s procedure [2,3,5].
Pancreatic lipoma is a rare benign mesenchymal tumor. It mostly occurs in the head of the pancreas. It is usually asymptomatic and discovered incidentally. In that case, it can be managed conservatively and monitored. However, an exact radiological diagnosis differentiating it from a well-differentiated liposarcoma or other fat-containing tumors can be difficult.
Authors’ contributions: All the authors have contributed equally to the data collection, interpretation, and preparation of the manuscript.
Patient’s consent: For the publication of this case report, written informed consent was obtained from the patient.
- Walker BS, Davis JL, Mayo SC. Large Pancreatic Lipoma Causing Duodenal Obstruction. J Gastrointest Surg. 2021 Apr;25(4):1070-1072. doi: 10.1007/s11605-020-04773-6. Epub 2020 Aug 10. PMID: 32779086.
- Lee SY, Thng CH, Chow PKh. Lipoma of the pancreas, a case report and a review of the literature. World J Radiol. 2011 Oct 28;3(10):246-8. doi: 10.4329/wjr.v3.i10.246. PMID: 22229078; PMCID: PMC3252557.
- Xiao RY, Yao X, Wang WL. A huge pancreatic lipoma mimicking a well-differentiated liposarcoma: A case report and systematic literature review. World J Clin Cases. 2019 Aug 26;7(16):2352-2359. doi: 10.12998/wjcc.v7.i16.2352. PMID: 31531331; PMCID: PMC6718797.
- Alzarie MF, Alhaddab AA, Aljafar FA, Alzahrani MM, Abdelaziz DM, Aleidan AA, Alduraibi KI, Alfawaz MA, Khoja MT, Alshahrani AA, Alhassoun HY, Alshaibi AM, Alghizzi AA, Aljohani MD, Al-Hawaj F. Lipoma of the Pancreas: A Rare Incidental Tumor. Cureus. 2021 Dec 2;13(12):e20122. doi: 10.7759/cureus.20122. PMID: 35003962; PMCID: PMC8723728.
- Lee JY, Seo HI, Park EY, Kim GH, Park DY, Kim S. Histologic confirmation of huge pancreatic lipoma: a case report and review of literatures. J Korean Surg Soc. 2011 Dec;81(6):427-30. doi: 10.4174/jkss.2011.81.6.427. Epub 2011 Nov 25. PMID: 22200046; PMCID: PMC3243862.
- Hasbahceci M, Erol C, Basak F, Barman A, Seker M. Incidental pancreatic lipomas diagnosed by computed tomography. Eurasian J Med. 2014 Feb;46(1):22-5. doi: 10.5152./eajm.2014.04. PMID: 25610289; PMCID: PMC4261445.
- Beddi A, Merzem A, Harmak M, Belgadir H, Amriss O, Moussali N, El Benna N. Pancreatic Lipoma: A Pancreatic Incidentaloma Diagnosis with Computed Tomography. Eur J Case Rep Intern Med. 2021 Mar 23;8(3):002252. doi: 10.12890/2021_002252. PMID: 33869089; PMCID: PMC8046283.
- Kishan TV, Pavithra S, Sri Bhuvana N, Kotha VK, Moorthy RS. A rare tumour of pancreas in an incidentally discovered pancreatic lipoma. Med J Armed Forces India. 2015 Jul;71(Suppl 1):S138-40. doi: 10.1016/j.mjafi.2013.09.010. Epub 2013 Nov 20. PMID: 26265810; PMCID: PMC4529551.