
More Information
Submitted: October 14, 2021 | Approved: October 18, 2021 | Published: October 19, 2021
How to cite this article: Ayadi MF, Hajri M, Talbi G, Mestiri H, Bayar R. Surgical management of splenic tuberculosis with pleural fistulation in a COVID-19 patient. Arch Case Rep. 2021; 5: 027-027.
DOI: 10.29328/journal.acr.1001052
Copyright License: © 2021 Ayadi MF, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Surgical management of splenic tuberculosis with pleural fistulation in a COVID-19 patient
Mohamed Firas Ayadi, Mohamed Hajri*, Ghofran Talbi, Hafedh Mestiri and Rached Bayar
Department of General Surgery, Mongi Slim University Hospital, La Marsa, Tunis, Tunisia
*Address for Correspondence: Mohamed Hajri, Department of General Surgery, Mongi Slim University Hospital, La Marsa, 26, Rue Essamaouel, Mutuelle Ville, Tunis, Tunisia, Email: [email protected]
A 38-year-old woman with no past medical history presented to the emergency room with dyspnea, fever and upper left abdominal pain. His respiratory rate was 28 breaths/min and his oxygen saturation was 91% on room air, improving to 96% on 6L/min oxygen via a non-rebreathing mask. Reverse transcription (RT)-PCR analysis of COVID-19 was positive. Laboratory investigations were within normal limits. Chest and abdominal CT scan revealed a large solitary splenic lesion with a pleural effusion. The diagnosis of splenic abscess with consecutive pleural empyema was strongly suspected. Chest tube drain was inserted and brought back a gelatinous fluid. Emergency surgery was decided for both therapeutic and diagnostic purposes. Intraoperatively, a large granulomatous splenic lesion was found and was centered by caseous necrosis (Figure 1). Splenectomy was performed. The postoperative course was uneventful. Histopathological examination of the specimen supported the diagnosis of splenic tuberculosis. The patient is actually under anti-tuberculosis drugs.
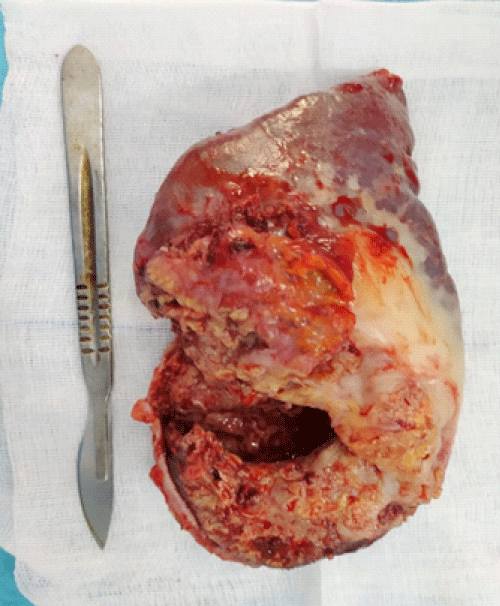
Figure 1: Splenectomy specimen showing granulomatous lesions with caseous necrosis.
Splenic tuberculosis is extremely rare and has no characteristic symptoms [1]. Therefore, diagnosis delays may be seen and can lead to fatal complications [2]. Both the coronavirus disease 2019 (COVID-19) and tuberculosis are transmitted through the respiratory route and affect the lungs [3]. Some studies suggest a link between the tuberculosis-COVID-19 coinfection and poor outcomes especially in immunosuppressed individuals [4–6].
- Raviraj S, Gogia A, Kakar A, Byotra SP. Isolated splenic tuberculosis without any radiological focal lesion. Case Rep Medi. 2015; 2015: 130209. PubMed: https://pubmed.ncbi.nlm.nih.gov/25628658/
- Gupta A. Splenic tuberculosis: a comprehensive review of literature. Pol Przegl Chir. 2018; 90: 49–51. PubMed: https://pubmed.ncbi.nlm.nih.gov/30426945/
- Fuady A, Houweling TA, Richardus JH. COVID-19 and tuberculosis-related catastrophic costs. The Am J Trop Med Hyg. 2021; 104: 436-440. PubMed: https://pubmed.ncbi.nlm.nih.gov/33269683/
- Stochino C, Villa S, Zucchi P, Parravicini P, Gori A, et al. Clinical characteristics of COVID-19 and active tuberculosis co-infection in an Italian reference hospital. Eur Respir J. 2020; 56: 2001708. PubMed: https://pubmed.ncbi.nlm.nih.gov/32482787/
- Vanzetti CP, Salvo CP, Kuschner P, Brusca S, Solveyra F, et al. Tuberculosis and COVID-19 coinfection. Medicina (B Aires). 2020; 80: 100–103. PubMed: https://pubmed.ncbi.nlm.nih.gov/33481740/
- Mishra A, George AA, Sahu KK, Lal A, Abraham G, et al. Tuberculosis and COVID-19 Co-infection: An Updated Review. Acta Biomed. 2020; 92: e2021025. PubMed: https://pubmed.ncbi.nlm.nih.gov/33682808/