
More Information
Submitted: 29 August 2020 | Approved: 07 September 2020 | Published: 08 September 2020
How to cite this article: Hajri M, Ferjaoui W, Atallah A, Bacha D, Bayar R, et al. Exceptional intraoperative aspects of mesenteric venous gas. Arch Case Rep. 2020; 4: 050-051.
DOI: 10.29328/journal.acr.1001042
ORCiD: orcid.org/0000-0002-4279-9370
Copyright License: © 2020 Hajri M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Exceptional intraoperative aspects of mesenteric venous gas
Mohamed Hajri1, Wael Ferjaoui1*, Aziz Atallah1, Dhouha Bacha2, Rached Bayar1 and Mohamed Tahar Khalfallah1
1Department of General Surgery, Mongi Slim University Hospital, Faculty of Medicine
of Tunis, Tunisia
2Department of Pathology, Mongi Slim University Hospital, Faculty of Medicine of
Tunis, Tunisia
*Address for Correspondence: Wael Ferjaoui, Department of General surgery, Mongi Slim University Hospital, Faculty of Medicine of Tunis, Tunisia, Tel: +216 52430099; E mail: [email protected]
A 73-year-old female patient presented to the emergency department with a 3-day history of acute abdominal pain and diarrhea. She had also a history of hypertension, type 2 diabetes mellitus and hypercholesterolemia. Physical examination revealed examination a generalized abdominal tenderness with an important abdominal distension, with a body temperature of 37.5°, a pulse rate of 115 bpm and a blood pressure of 105/65 mmHg. Laboratory data showed white blood cells at 15.500/mm³, C-reactive protein at 155 mg/l, hemoglobin at 12.3 g/dl and creatinine at 105 µmol/l. Chest radiography was normal. Contrast enhanced CT of the abdomen revealed hepatic portal venous gas with diffuse gas accumulation in the branches of the superior mesenteric vein, gaseous distention of the small bowel with reduced enhancement of the bowel wall (Figure 1). Additionally, an atheromatous obstruction was observed in the superior mesenteric artery at 4cm from its origin (Figure 2). Emergency surgery was decided. Extensive bowel infarction was observed and no mesenteric artery pulse was detected. We was impressed by the exceptional intraoperative aspects of gas accumulation in the superior mesenteric vein (Figure 3). No such image has been published in the literature. Therapeutic abstention was decided. Patient died shortly afterwards.
Hepatic portal venous gas is a rare radiological sign which carries a worse prognosis. It’s associated with numerous underlying abdominal disease [1]. Advanced bowel infarction is the most frequent cause, but it can be present in other conditions like ulcerative colitis, intraabdominal abscess, small bowel obstruction, and gastric ulcers [2]. The diagnosis is usually made by computed tomography, and often shows advanced disease [3]. The originality of our case consists in the intraoperative aspect of the mesenteric venous gas which has never been published in the literature.
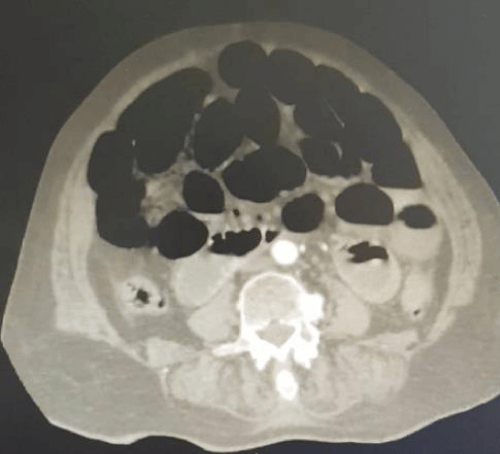
Figure 1: CT scan images of small bowel distention with reduced enhancement of the bowel wall.
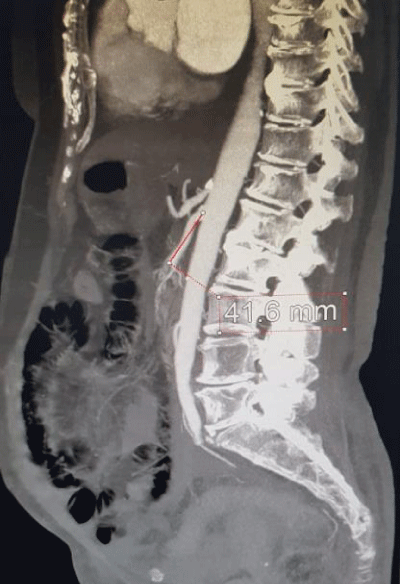
Figure 2: CT scan images of superior mesenteric vein obstruction.
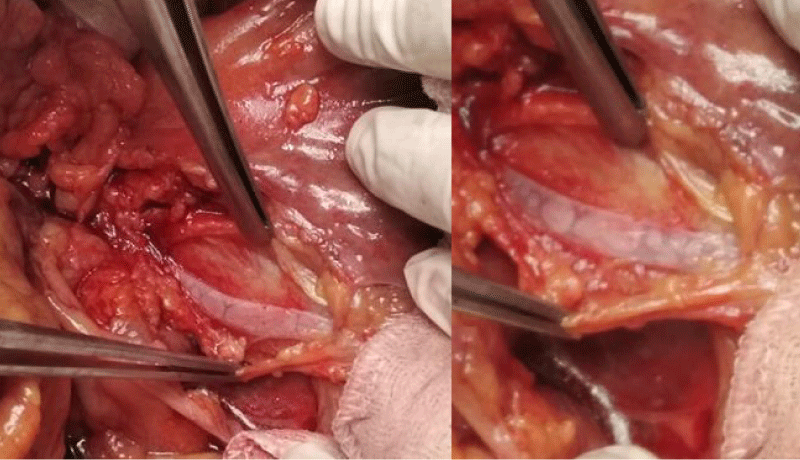
Figure 3: Intraoperative aspect of gas accumulation in the superior mesenteric vein.
- Abboud B, El Hachem J, Yazbeck T, Doumit C. Hepatic portal venous gas: physiopathology, etiology, prognosis and treatment. World J Gastroenterol. 2009; 15: 3585-3590. PubMed: https://pubmed.ncbi.nlm.nih.gov/19653334/
- Chen H, Zhan S, Deng Q, Hong C, Chen J, et al. Hepatic portal venous gas associated with bowel necrosis: report of one case and literature review. Digestive Med Res. 2020; 3: http://dmr.amegroups.com/article/view/5690
- Nelson AL, Millington TM, Sahani D, Chung RT, Bauer C, et al. Hepatic portal venous gas: the ABCs of management. Arc Surg. 2009; 144: 575‑581. PubMed: https://pubmed.ncbi.nlm.nih.gov/19528392