
More Information
Submitted: June 09, 2025 | Approved: June 18, 2025 | Published: June 19, 2025
How to cite this article: Gnanaselvam P, Pathiragoda GDD, Wickramaratne SE, Mathivannan G, Karunanithy P. A Rare Case of Mechanical Small Bowel Obstruction Secondary to Herniation of a Part of the Ileum through a Defect in the Meso-appendix with Appendicitis and its Laparoscopic Management. Arch Case Rep. 2025; 9(6): 204-206. Available from:
https://dx.doi.org/10.29328/journal.acr.1001147
DOI: 10.29328/journal.acr.1001147
Copyright license: © 2025 Gnanaselvam P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Small bowel obstruction; Mesoappendix; Appendicitis; Laparoscop

A Rare Case of Mechanical Small Bowel Obstruction Secondary to Herniation of a Part of the Ileum through a Defect in the Meso-appendix with Appendicitis and its Laparoscopic Management
Pamathy Gnanaselvam*, Gabadage Don Harsha Dishantha Pathiragoda, Saranga Eshanie Wickramaratne, G Mathivannan and Pirahanthan Karunanithy
Department of Surgery, National Hospital of Sri Lanka, Colombo 10, Sri Lanka
*Address for Correspondence: Pamathy Gnanaselvam, Department of Surgery, National Hospital of Sri Lanka, Colombo 10, Sri Lanka, Email: [email protected]
Small Bowel Obstruction (SBO) resulting from internal herniation through a defect in the mesoappendix is extremely rare, with only a few documented cases found in the literature in the context of acute appendicitis. We are presenting a case of a 79-year-old female who presented with atypical abdominal pain with a history of a fall. Due to persistent abdominal pain and tenderness on examination, further investigations were conducted. A Computed Tomography (CT) scan revealed SBO with a transition point at the terminal ileum, suspected to be caused by adhesions or mesenteric twisting. Laparoscopic exploration identified a herniated loop of the bowel through a defect in the mesoappendix, alongside an inflamed appendix containing fecaliths. The obstruction was successfully relieved via a laparoscopic approach, with an appendectomy performed concurrently. The postoperative period was uncomplicated. This case underscores the importance of considering rare causes of intestinal obstruction, particularly when clinical presentation is atypical. Early diagnosis and timely surgical intervention are crucial for favorable outcomes. In cases of SBO, rare pathologies should always be considered before making surgical decisions. This case also highlights the importance of considering the length of appendix and its associated risks in mechanical obstruction.
Intestinal obstruction is a common cause of acute abdomen with a wide range of potential etiologies. Mechanical small bowel obstruction is a very rare occurrence in acute appendicitis [1]. The association between acute appendicitis and mechanical intestinal obstruction was first described by Hotchkiss et al. in 1901 and later by Hawkes in 1909 [2,3]. While the typical presentation of appendicitis involves functional obstruction, in very rare cases, it may present as a mechanical obstruction, particularly in the form of a closed-loop obstruction. The clinical features of small bowel obstruction can obscure the clinical picture of appendicitis [1]. Diagnosis of acute appendicitis is established via diagnostic modalities, such as Computed Tomography (CT) of the abdomen or diagnostic laparoscopy while it is currently best treated by laparoscopic intestinal obstruction release with appendicectomy.
A 79- year- old female following accidental fall transferred to Teaching hospital for tertiary care with NCCT brain and Geriatric assessment. She had a history of hypertension, dementia and total abdominal hysterectomy with bilateral salpingooophorectomy 10 yrs ago due to endometrial carcinoma. With the history of lower abdominal pain for one day duration, on examination tenderness over lower abdomen and epigastric area, along with audible bowel sounds were noted. Neurological examination was unremarkable except for positive cerebellar sign. A Contrast-enhanced CT scan revealed small bowel obstruction with transition point at terminal ileum (Figures 1-3) with suspected adhesions or mesenteric twist with minimal ascites. Laparoscopic exploration with possible intervention was decided upon, with the clinical and CT findings confirming intestinal obstruction. A closed bowel loop obstruction through a defect in the mesoappendix was noted, with an inflamed appendix containing a fecalith. There was a moderate amount of free fluid. Laparoscopic release of the intestinal obstruction and appendicectomy were performed (Figure 4). The procedure was uneventful, and the patient was discharged on the third postoperative day with no postoperative complications. Histology of the appendix confirmed an inflamed appendix.
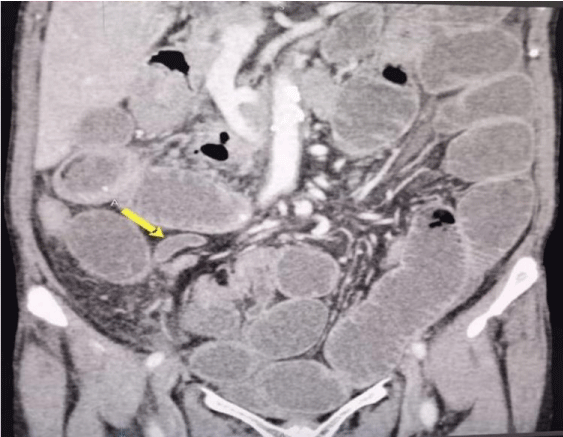
Figure 1: Coronal plane CECT showing Appendix [A].
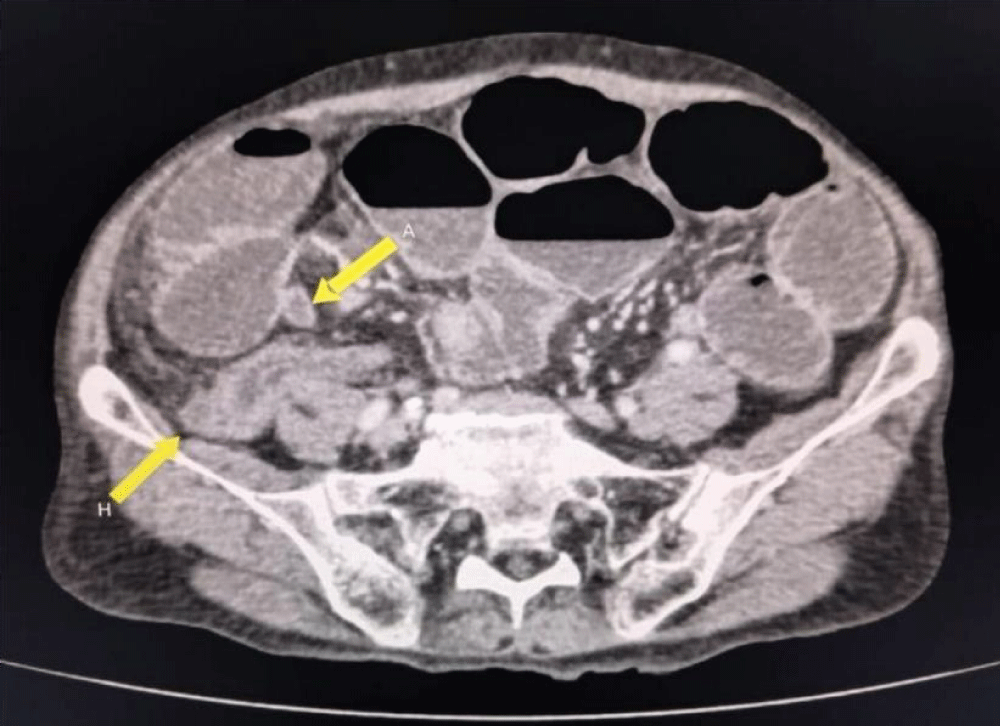
Figure 2: Axial CECT showing Appendix [A] and Hernia [H].

Figure 3: Sagittal plane CECT showing Appendix [A].
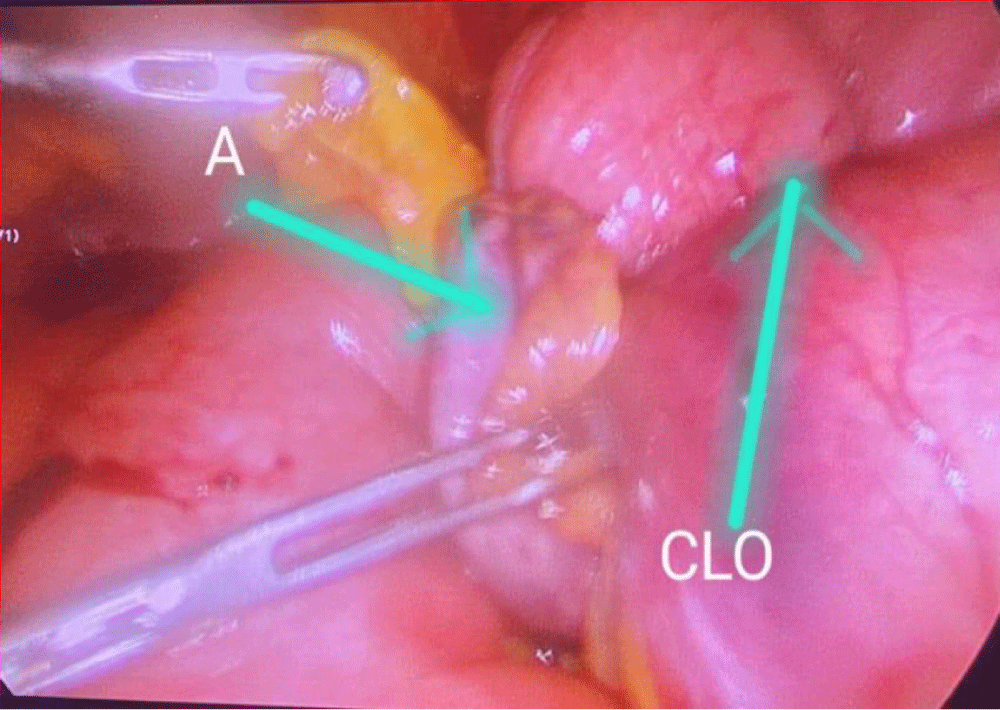
Figure 4: Intraoperative finding of appendix [A] and a closed loop obstruction [CLO].
Mechanical intestinal obstruction is a significant clinical entity resulting from various etiologies, including adhesions, hernias, and neoplasms. Internal herniation through a defect in the mesoappendix is an extremely rare cause of obstruction, with only a few cases documented in the literature. To date, we found only one case in the literature that was successfully managed laparoscopically [4].
In this patient, the presentation was atypical, not featuring the typical symptoms of intestinal obstruction such as abdominal pain, distension, and vomiting. This atypical presentation may partly be attributed to her history of dementia and recent fall. Initial diagnostic studies, including abdominal X-rays and CT scans, showed signs consistent with mechanical obstruction, but the exact cause remained elusive. It was only during exploratory laparoscopy that the defect in the mesoappendix and subsequent internal herniation were identified.
The mesoappendix is a peritoneal fold that surrounds the appendix and connects it to the peritoneal cavity, housing the appendicular artery and vein. A defect in this structure allows bowel loops to herniate, leading to obstruction. Due to its small size and limited mobility, significant herniation is uncommon. However, in this case, the patient’s appendix was unusually long (14 cm), increasing the likelihood of herniation through the mesoappendix (Figure 5). The average length of the vermiform appendix is generally 8 cm - 10 cm (3.5 inches) [5], although lengths up to 24.5 cm have been reported [6]. With increasing age, the length of the vermiform appendix tends to decrease [7]. As per a study conducted in Sri Lanka average length of appendix reported as 8.2cm [8]. Further research is needed to explore whether an increased appendix length correlates with a higher risk of appendicitis and mechanical obstruction.
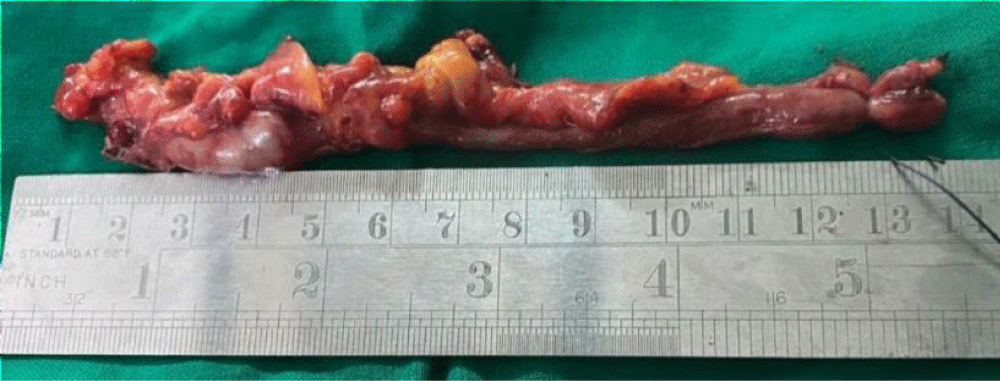
Figure 5: A length of the appendix of patient.
The pathophysiology of this condition may involve congenital or acquired defects in the mesoappendix. Congenital defects are related to developmental anomalies of the appendix, while acquired defects may result from previous surgeries, trauma, or inflammatory conditions like appendicitis.
Management of internal herniation requires urgent surgical intervention. While open laparotomy is commonly performed in cases of intestinal obstruction, this patient’s CT scan suggested adhesions or mesenteric twisting as potential causes of obstruction. Thus, a laparoscopic approach was utilized. The procedure was uneventful, and the patient was discharged on the third postoperative day. Laparoscopic management of mechanical intestinal obstruction due to internal herniation remains rare, with only one other case reported in the literature with laparoscopic management of mechanical intestinal obstruction due to the formation of encircling loop around a bowel segment [4]. Open laparotomy procedures are relatively common [9-18].
This case emphasizes the importance of considering rare causes of intestinal obstruction, particularly in patients with atypical presentations. It also highlights the potential role of exploratory surgery in identifying obscure causes of mechanical obstruction.
Internal herniation through a defect in the mesoappendix is a rare but one of the causes of mechanical intestinal obstruction that necessitates prompt surgical intervention. Awareness of this condition is critical for timely diagnosis and effective management.
- Awale L, Joshi BR, Rajbanshi S, Adhikary S. Appendiceal tie syndrome: A very rare complication of a common disease. World J Gastrointest Surg. 2015;7(4):67–70. Available from: https://doi.org/10.4240/wjgs.v7.i4.67
- Hotchkiss LWV. Acute intestinal obstruction following appendicitis. A report of three cases successfully operated upon. Ann Surg. 1901;34(5):660–77. Available from: https://doi.org/10.1097/00000658-190107000-00070
- Hawkes F III. The prevention of intestinal obstruction following operation for appendicitis. Ann Surg. 1909;49(2):192–207. Available from: https://doi.org/10.1097/00000658-190902000-00003
- Gupta P, Rajapandian S, Sabnis SC, Palanivelu C. Laparoscopic management of an unusual case of small bowel obstruction: appendiculoileal knotting. BMJ Case Rep. 2018;2018:bcr2018224640. Available from: https://doi.org/10.1136/bcr-2018-224640
- Bornali H, Sekhar DR. A study on length of human appendix in different ages. IJHRMLP. 2016;2(2):101-6. Available from: https://ijhrmlp.org/uploads/files/2_2_21_original_paper_bornali_hazarika.pdf
- Collins DC. The Length and Position of the Vermiform Appendix: A Study of 4,680 Specimens. Ann Surg. 1932;96(6):1044-8. Available from: https://doi.org/10.1097/00000658-193212000-00012
- Patel S, Naik A. Study of the length of vermiform appendix. Indian J Basic Appl Med Res. 2016;5:256-60. Available from: https://www.ijbamr.com/assets/images/issues/pdf/June%202016%20256%20-%20260.pdf
- Ekanayake PM, Amaratunga HA, Vadisinghe AN, Senasinghe P, Adikari SB. The position and morphology of the vermiform appendix in Sri Lankans: a study on autopsies. SLAJ. 2017;1(2):31-34. Available from: https://doi.org/10.4038/slaj.v1i2.36
- Ahmed KA, Hamdy AMF, Seifeldin MI, et al. Mechanical small bowel obstruction due to appendiceal tourniquet: a case report and review of literature. J Med Case Reports. 2019;13(1):208. Available from: https://doi.org/10.1186/s13256-019-2156-y
- Habib R, Zaib Z, Afzal MW, Habib R, Wasim M, Shah Afridi MN. APPENDICEAL TIE SYNDROME: A RARE CAUSE OF SMALL BOWEL OBSTRUCTION. J Ayub Med Coll Abbottabad. 2023;35(4):688-9. Available from: https://doi.org/10.55519/jamc-04-9649
- Blachar M, Federle MP, Dodson SF. Internal hernia: Clinical and imaging findings in 17 patients with emphasis on CT criteria. Radiology. 2001;218(1):68–74. Available from: https://doi.org/10.1148/radiology.218.1.r01ja5368
- Hashimoto D, Hirota M, Sakata K, Yagi Y, Baba H. Adult transmesenteric hernia: Report of two cases. Surg Today. 2012;42(5):489-92. Available from: https://doi.org/10.1007/s00595-011-0035-2
- Cutler GD. Mesenteric Defects as Cause of Intestinal Obstruction. Boston Med Surg J. 1925;192(7):305-11. Available from: https://www.nejm.org/doi/pdf/10.1056/NEJM192502121920708
- Lubat E, Gordon RB, Birnbaum BA, Megibow AJ. CT diagnosis of posterior perineal hernia. AJR Am J Roentgenol. 1990;154(4):761-2. Available from: https://doi.org/10.2214/ajr.154.4.2107672
- Mathie D, Luciani A. Internal abdominal herniations. AJR Am J Roentgenol. 2004;183(2):397–404. Available from: https://doi.org/10.2214/ajr.183.2.1830397
- Zissin R, Hertz M, Gayer G, Paran H, Osadchy A. Congenital internal hernia as a cause of small bowel obstruction: CT findings in 11 adult patients. Br J Radiol. 2005;78(933):796–802. Available from: https://doi.org/10.1259/bjr/87050272
- Rooney JA, Caroll JP, Keeley JL. Internal hernias due to defects in the mesoappendix and mesentry of small bowel and probable Ivemark syndrome: Report of two cases. Ann Surg. 1963;157(2):254-8. Available from: https://doi.org/10.1097/00000658-196302000-00011
- Barman S, Hadiuzzaman M, Ray S, Sarkar R. Internal herniation of Meckel’s diverticulum through meso appendix in infant: An extremely rare occurrence. CHRISMED J Health Res. 2016;3(1):89-91. Available from: https://journals.lww.com/chri/fulltext/2016/03010/internal_herniation_of_meckel_s_diverticulum.20.aspx